Nanoknife for the treatment of prostate cancer
The indications, benefits, risks, technique and post-operative course associated with prostate Nanoknife.
What is focal therapy?
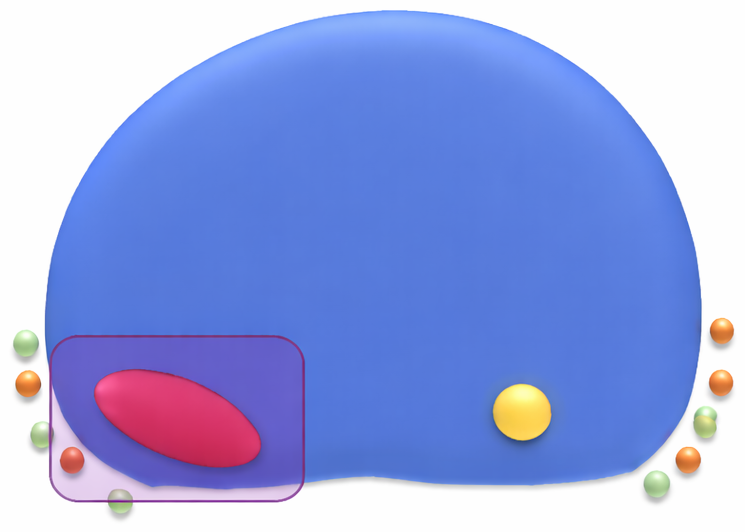
Focal Therapy involves treating 1-2 areas of cancer in the prostate so that less tissue is damaged. This means the cancer is treated but without causing collateral tissue damage to nerves, muscles, bladder and back passage. Recovery is quicker than radical surgery or radical radiotherapy as well. Focal therapy can be carried out using different energies which ablate (or destroy) tissue precisely. One of these is Nanoknife.
What is prostate cancer?
The prostate is actually part of the male reproductive system. It is a walnut-sized gland in the male reproductive system just below the bladder. It surrounds part of the urethra, the duct that empties the bladder.
The main function of the prostate is to supply fluid for the sperm during ejaculation. Prostate Specific Antigen (PSA) is produced by the prostate gland.
Prostate cancer begins when the cells in the prostate start to divide and grow out of their normal pattern. The cells that are growing are similar to cells in the prostate, but they do not grow into normal prostate tissue. They grow into lumpy bundles of cells called tumours. Tumours disrupt the normal function of the prostate, and cells that come free from the tumour can travel elsewhere in the body, and begin to grow tumours there. Prostate cancer may be localised (only affecting the prostate), or it may be locally advanced (spread outside the outer capsule of the prostate but not into the blood stream) or metastatic (the cancer has moved outside the prostate and into the bloodstream and may affect other organs). Your surgeon will be able to discuss what type of tumour you have and the likelihood of this spreading. The treatment recommended will depend on the size and site of your tumour.
What does “Nanoknife for Localised Prostate Cancer” mean?
Prostate Nanoknife is a surgical technique that can be used to treat cancer that has not spread outside the prostate. Nanoknife aims to use high voltage electricity directed at the cancer area to destroy the prostate cancer cells.
Who is suitable and how can prostate Nanoknife help?
You may be suitable for prostate Nanoknife treatment if you have localised prostate cancer – that is, the cancer has been shown to be within the prostate only.
We first have to perform scans to visualise where the cancer is in your prostate and to ensure the cancer is confined to the prostate and has not spread outside it. We will then take a biopsy or tissue from your prostate to obtain definite evidence that there is cancer. We also take into account information from PSA (prostate specific antigen) measurements (PSA is a substance released into the blood by prostate and prostate cancer cells). If there is evidence that the cancer has spread outside the prostate then you may be informed that you are not suitable for Nanoknife treatment.
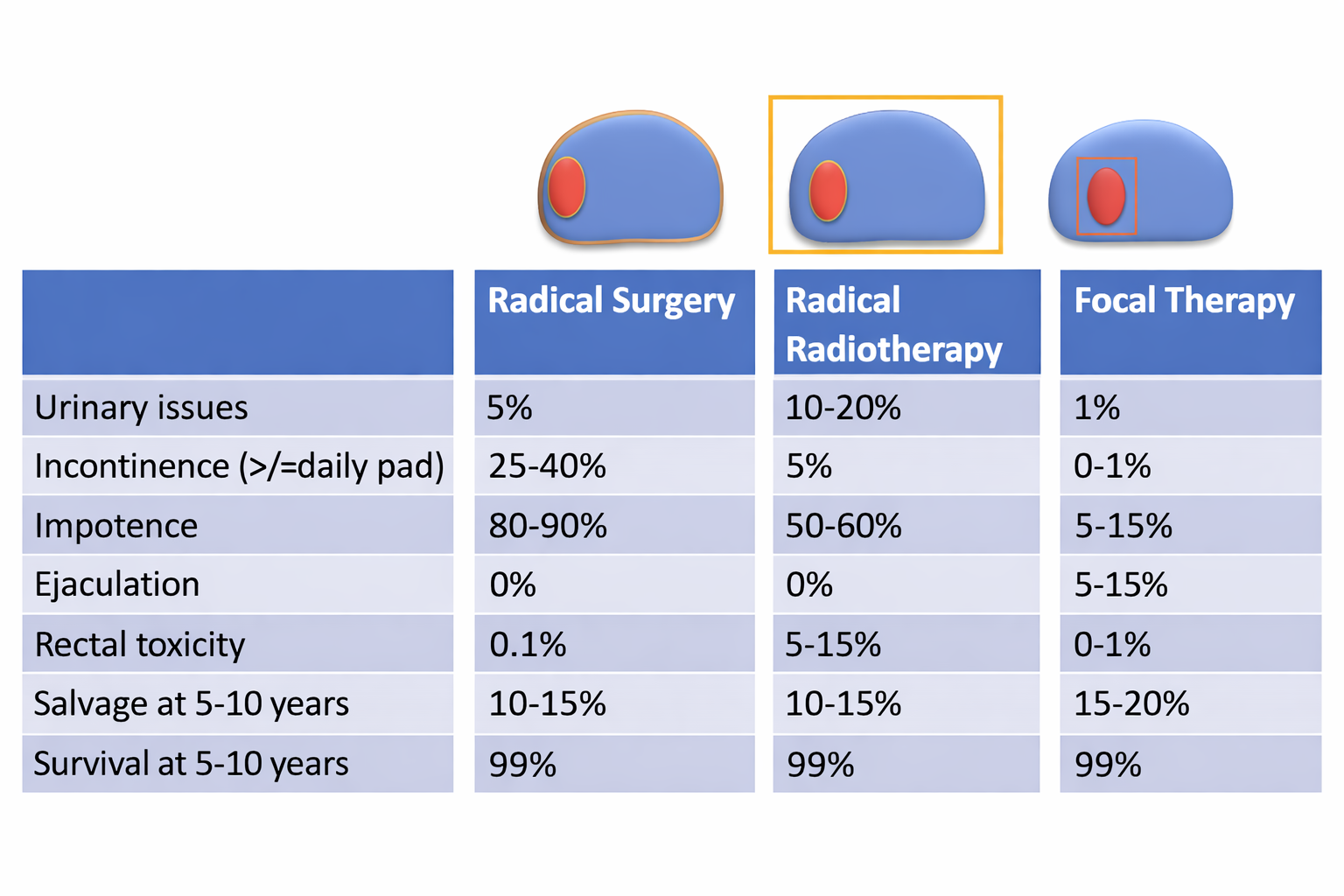
The cure rates reported after surgery and radiotherapy are between 80- 85% at 10 to 15 years. What this means is that 80 to 85% of men receiving either treatment had no evidence of prostate cancer whilst they were being monitored. The Nanoknife results are similar to this in the medium term. We do not know what the Nanoknife cure rates at 10 to 15 years are as it is a relatively new treatment.
In addition, Nanoknife can be repeated and about 1 in 5 to 1 in 4 men need a second Nanoknife treatment.
The benefits of Nanoknife for localised prostate cancer include:
- The treatment can potentially cure the cancer
- It is a minimally invasive treatment (no incisions)
- A short hospital stay (you will either go home the same day or stay in hospital for one night)
- A rapid recovery, which means that you can return to daily living quickly
- A low rate of side-effects especially when used as a focal therapy (to treat just the tumour and not the whole prostate)
What are the risks of Nanoknife for localised prostate cancer?
All treatments and procedures have risks and we will talk to you about the risks of Nanoknife for localised prostate cancer.
Problems that may happen straight away:
- A small number of men have difficulty in passing urine after the treatment and will need a tube (catheter) to be inserted to help with this. This is usually left for around 2 weeks, then removed.
- Some men will notice swelling of their penis or scrotum, which may happen in the first or second week after the procedure. This is temporary and will usually resolve within two months.
- A few men may develop tingling or numbness around the penis. This is a temporary side effect and will usually resolve within two to four months.
- Pain around or in the rectum (back passage) can occur in up to 18 out of every 100 men following treatment. This usually settles within 3 months.
Problems that may happen later:
- Impotence / erectile dysfunction (problems getting or maintaining an erection). Many men may already have pre-existing impotence as a result of other problems. However, because the nerves involved in creating an erection lie around the prostate gland, they might be affected during the electroporation process. When Nanoknife is used to treat just the area of important cancer – this is called focal therapy – then the risk of impotence is lower at around 5-10 men out of every 100 men treated who have good erections. There are some treatments available on the NHS such as tablets and injections that can help to restore erections for some men, but not all.
- Urine incontinence (leakage of urine). Leakage of urine can occur in 1 to 2 out of every 100 men after treatment. This may improve with time. Some men may need to wear pads to protect their underwear. We teach pelvic floor exercises to help your urinary control.
Problems that are rare, but serious:
- A rare complication of prostate Nanoknife is a connection forming between the back passage (rectum) and the tube which carries the urine (urethra). This is known as a fistula and is due to the back passage being damaged during the Nanoknife treatment. This complication occurs in 1 in 1000 men treated. Although rare, this complication is serious and may require an operation to repair the hole. A “stoma”, where bodily waste is collected in an external bag worn on the body may occasionally be required.
What are the risks of the general anaesthetic?
Nanoknife treatment is given under a general anaesthetic. There are a number of issues that affect the chances of suffering complications from a general anaesthetic, including age, weight, lifestyle issues (e.g. smoking) and your general state of health. Your doctor can give further details.
The information below is provided by the Royal College of Anaesthetists:
Very common (1 in 10) and common (1 in 100) side effects:
- Feeling sick and vomiting after surgery
- Sore throat
- Dizziness, blurred vision
- Headache
- Itching
- Aches, pains and backache
- Pain during injection of drugs
- Bruising and soreness
- Confusion or memory loss
Uncommon side effects and complications (1 in 1000):
- Chest infection
- Bladder problems
- Muscle pains
- Slow breathing (depressed respiration)
- Damage to teeth, lips or tongue
- An existing medical condition getting worse
- Awareness (becoming conscious during your operation)
Rare (1 in 10,000) or very rare (1 in 100,000 or less) complications:
- Damage to the eyes
- Serious allergy to drugs
- Nerve damage
- Death
- Equipment failure
Deaths caused by anaesthesia are very rare, and are usually caused by a combination of four or five complications together. There are approximately five deaths for every million anaesthetics in the UK.
What will happen if I choose not to have prostate Nanoknife?
If you choose not to have prostate Nanoknife then other alternative treatments are available (refer to next section below), which the team will go through with you.
What alternatives are available?
At the time of diagnosis, prostate cancer may be confined to the prostate itself, or may have spread to other sites within the body. If prostate cancer is confined to the prostate, it may be possible to cure it. The types of treatment that for prostate cancer when it is confined to the prostate include the following:
- Active surveillance
- HIFU
- Cryotherapy
- External beam radiotherapy
- Brachytherapy (small implanted radioactive seeds)
- Surgery (radical prostatectomy)
You may or may not be suitable for these treatments. Your doctor will tell which of these you are suitable for and discuss the advantages and disadvantages of each. Often, your doctor will not know which treatment is better for you and you will be asked to choose which treatment you would like to have.
What is the difference between HIFU, Cryotherapy and Nanoknife?
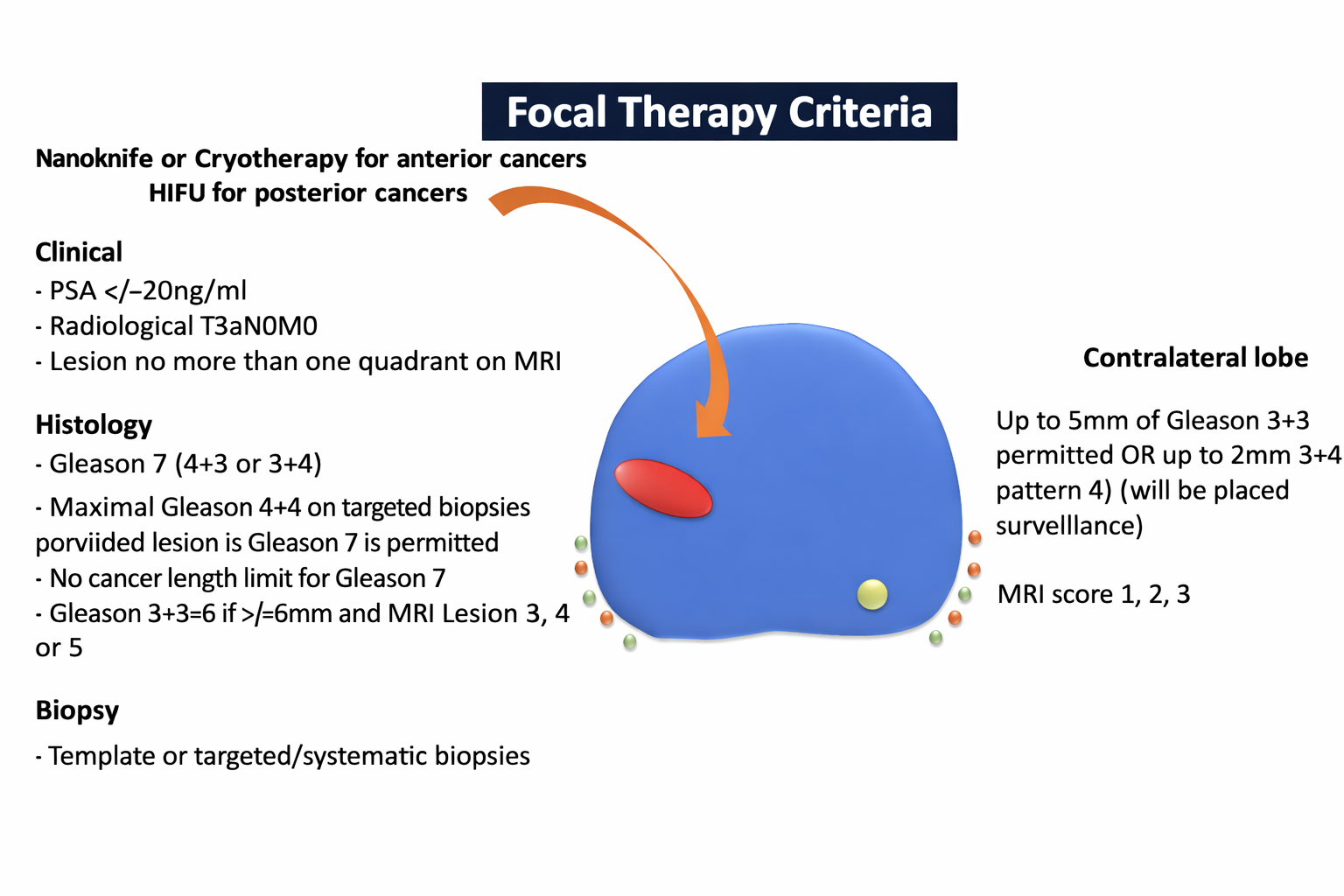
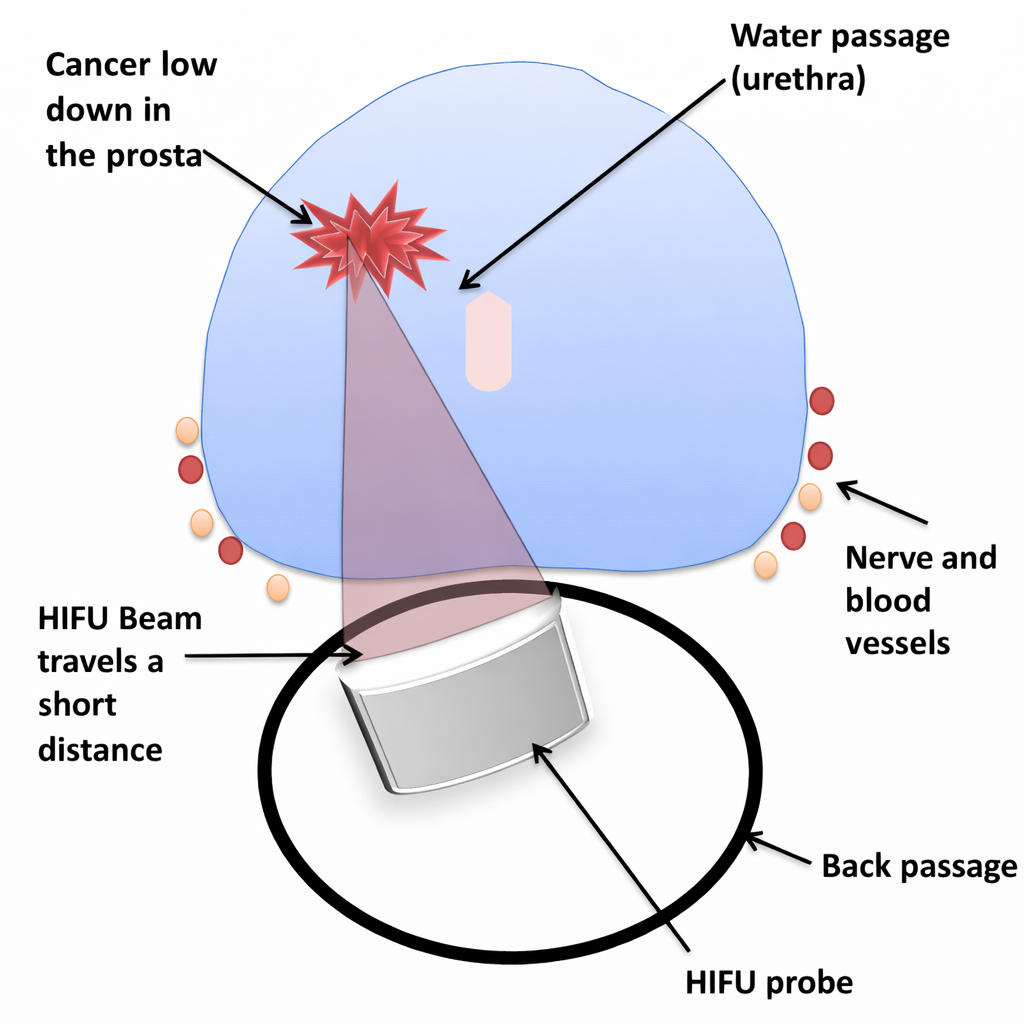
High intensity focused ultrasound treatment (HIFU) uses ultrasound to heat tissue. Cryotherapy uses freezing to kill tissue. Nanoknife uses high voltage electricity to destroy tissue. Your doctor will make a decision between HIFU, cryotherapy and Nanoknife using information about where your tumour is and whether there are any small stones (called calcifications) inside the prostate. Prostate calcifications can affect the effectiveness of the HIFU treatment if they are between the tumour and the HIFU probe. The position of the tumour in the prostate is also important. It can sometimes be more difficult to treat some tumours in the prostate that are further away from the HIFU probe. The HIFU probe sits in the back passage and the sound-waves travel through tissue to reach their target.
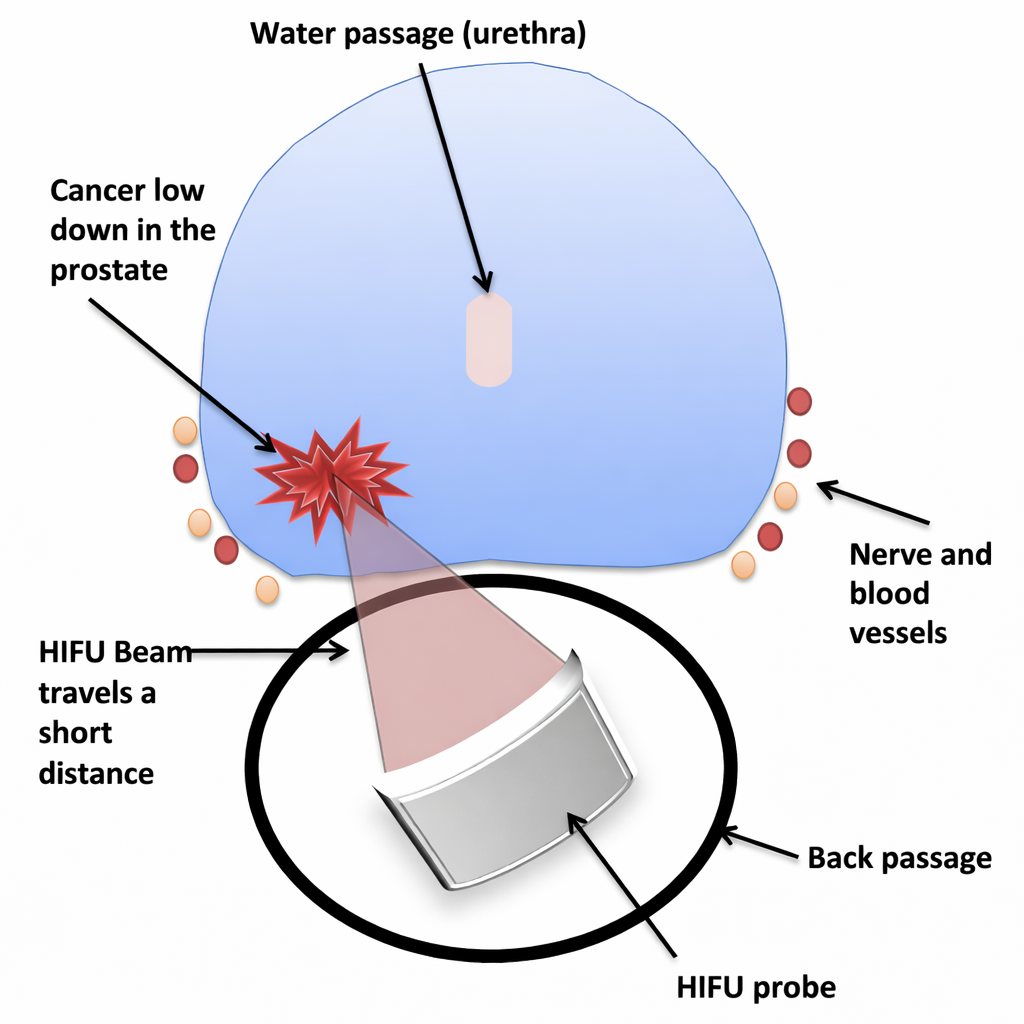
The more tissue there is the less energy that gets through. This can sometimes mean that it can be less effective for tumours in the areas furthest away from the back-passage. These are called anterior tumours.
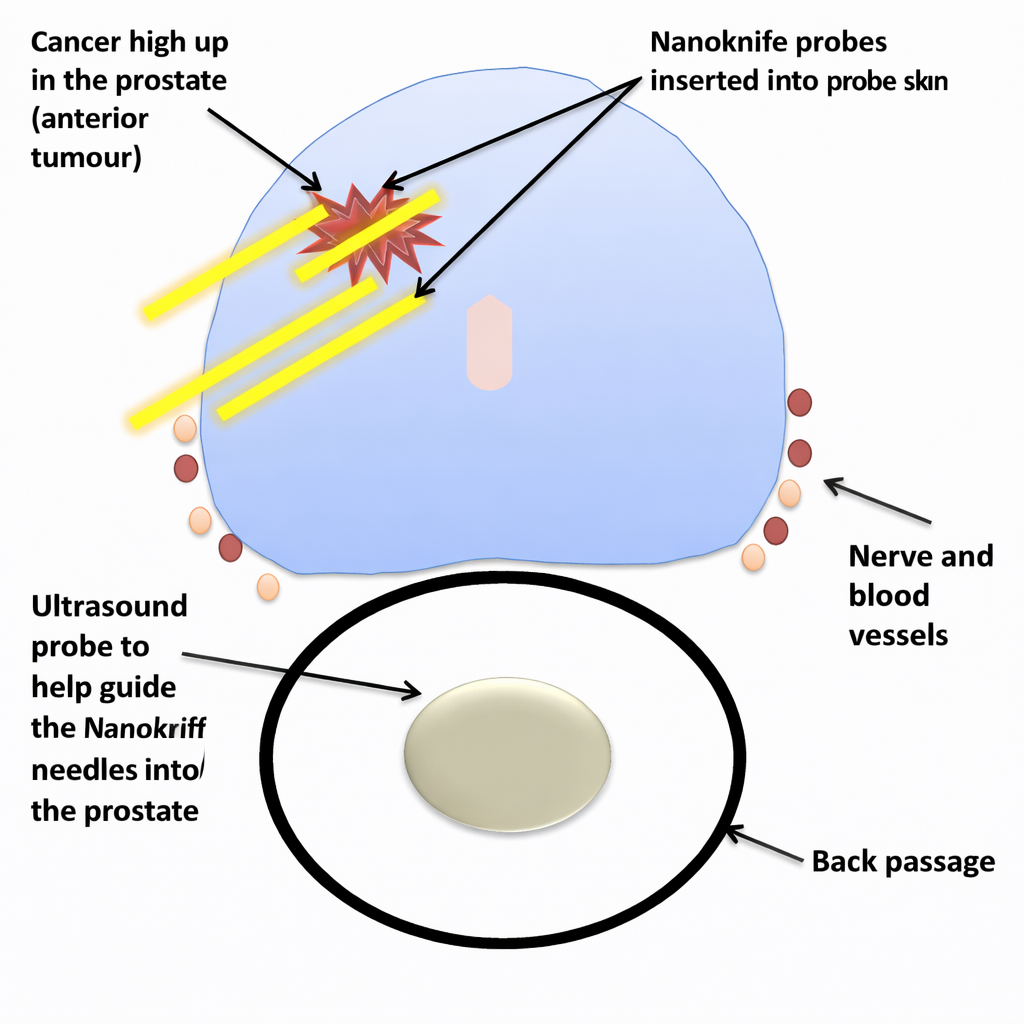
Cryotherapy and Nanoknife involve the needles being placed directly into the tumour and so the energy is applied closer to the tumour. These two treatments are used for cancers in the anterior areas of the prostate (furthest away from the rectum). The decision between the two of these is something that is made by your surgeon and not something for you to choose. This is because there are technical concerns that your surgeon will need to consider.
What will happen if I do not have any treatment?
This depends on the risk category of your disease. High risk categories of prostate cancer usually require some form of treatment. In this case, if you do not have treatment then the risk to you in terms of the cancer progressing is high. Delay in this instance may mean that treatment cannot be given at a later date and it could also mean that there is a risk to your life without any treatment.
Studies have shown that men who are in a low risk group (and some medium risk men) can be safely managed by active surveillance for a number of months to years and if they show signs of progression they can have treatment at that point. In fact, the difference between no treatment and radical prostatectomy is between 0% and 5% in terms of surgery reducing the chance of dying from prostate cancer over 10 years. Many men who choose treatment do not like the thought of having no treatment for cancer, so they choose a form of treatment that they want. Your doctor will have told you what risk category you are in. If you are unsure please ask your doctor or nurse practitioner to explain.
How should I prepare for prostate Nanoknife?
You will be given an appointment for an assessment with a nurse weeks before your operation. As part of this you will be given instructions as regards what you should bring with you on the day of the operation, whether you should continue taking all your medications as normal, what time you should arrive on the day and for how long you should fast before your arrival. On the actual day of the operation you will be given an enema 1 – 2 hours prior to the procedure. This involves putting liquid in your back passage to empty it, which allows us to obtain a clear ultrasound picture during the Nanoknife treatment.
The Nanoknife treatment takes approximately 1-2 hours under general anaesthetic (this means you will be asleep) and you will be able to go home the same day providing that there is someone to accompany you on the way home. Occasionally we may ask you to stay overnight if you do not have an escort to take you home or if you have medical problems that necessitate you having to remain in hospital.

Asking for your consent
We want to involve you in all the decisions about your care and treatment. If you decide to go ahead with prostate Nanoknife, by law we must ask you to sign a consent form before proceeding with the treatment. This confirms that you agree to have the procedure and understand what it involves. Staff will explain all the risks, benefits and alternatives before they ask you to sign a consent form. If you are unsure about any aspect of your proposed treatment, please don’t hesitate to speak with a senior member of staff again.
What happens during a prostate Nanoknife procedure?
IRE treats prostate cancer focally using pulses of electricity which create tiny holes in cancer cells, causing them to die. The low energy direct current (LEDC) can be very finely pinpointed. This makes this method highly accurate and explains its commercial name: NanoKnife. The treatment takes about 1 to 2 hours. During IRE, special needles or probes are passed into the prostate through the perineum. This is done in a similar manner to the prostate biopsy you had. Your doctor will use ultrasound images of the prostate to confirm that the needles are in the correct position.
A catheter (a narrow, flexible hollow tube inserted through the penis into the bladder) for urine drainage is left in place for 1–2 weeks after the procedure. Sometimes we have to place a suprapubic catheter – this is a catheter that is inserted through the skin of your lower abdomen (tummy) directly into the bladder.
What should I expect after prostate Nanoknife?
When you get home from the hospital after the Nanoknife treatment you should, at first, only perform small tasks and take plenty of rest in between. You should drink normal amounts of fluid every day – water is best and fruit juice is also acceptable but tea and coffee do not count. If there is dark or blood stained urine, increase your drinking amount. This will prevent you from becoming dehydrated and developing a urine infection or a blood clot forming that can block the catheter. Also, you should avoid constipation as this leads to straining. To help with this you will be given a gentle laxative syrup when you leave the hospital, e.g., lactulose (instructions will be provided as regards how much and how often you should take this). The laxative softens the stool (bowel movement) making it easier to pass. As regards the Nanoknife needle puncture sites in the skin in front of your anus (back passage), you should simply aim to keep this area clean and dry (no dressings should be needed in this area once you leave the hospital).
If there are any problems, call your doctor or GP or go to the nearest Accident and Emergency Department (Casualty). You should be aware of the following:
Urinary catheter
You will be discharged from hospital with a urinary catheter which will be left in place for 1–2 weeks after the procedure. You will be given instructions when and where to go to have this catheter removed. Before leaving hospital, the nurses will show you how to empty and change the catheter bag. The catheter should not cause you any discomfort. Intermittently, you may have the sensation of needing to pass urine. This is normal. Occasionally, the catheter may become blocked. Symptoms include pain in the lower tummy and inability to pass urine. This can be due to debris in the urine which in turn can be caused by a urine infection.
Pain
It is normal to expect some discomfort after your Nanoknife treatment particularly in and around the area that the Nanoknife needles were inserted. You will be provided with some simple pain killers on discharge from hospital and you can get more from your general practitioner if necessary.
Bleeding
Occasionally, there may be slight bleeding from the area in front of your anus (back passage) where the needles or probes used for Nanoknife were inserted (this area is termed the perineum). If this is happens, then you can apply a dry dressing. If the bleeding is heavier than slight, contact your doctor or GP or go to the nearest Accident and Emergency Department (Casualty).
Urine infection
Occasionally you may develop a urine infection following prostate Nanoknife. Symptoms may include fever, pain around your lower back or lower tummy, or pain on passing urine. If you develop any of these symptoms, you should contact your doctor, GP go to the nearest Accident and Emergency Department (Casualty).
Bruising and swelling of scrotum
You may develop some bruising in the area that the Nanoknife needles were inserted (perineum) or you may get some swelling of your scrotum after the procedure. Both of these will settle without any treatment over a couple of months.
Going home after Nanoknife
Most people recover to normal activities from the Nanoknife treatment within 1-2 weeks. In the days after the operation, you will probably feel more tired than usual, usually because of the anaesthetic, and as the body starts to heal the prostate. You do not need to be bed bound or house bound.
Your urine may be blood stained whilst you have your catheter, and you may also notice some tissue fragments in your urine (this may continue on-and-off for up to two months after your treatment). You might pass blood or blood clots. If this happens, drink plenty of water and it will clear. Rarely, the bleeding may continue in which case you should seek advice from your doctor or local emergency department.
If you have any of the following symptoms, contact your doctor or GP or go to your local Accident & Emergency department (casualty):
- Heavy and/or continuous bleeding
- A fever
- Pain that is not controlled by simple painkillers
Having your catheter removed
The catheter has a balloon at the tip inside holding it in the bladder. This often gives you a sensation of needing to pass urine even though the bladder is empty and urine is draining through the catheter. Sometimes the sensation can be very strong and sometimes the bladder spasms as a result, forcing urine around the catheter. This can be disconcerting and usually settles after 1-2 days. If it is does not, or you are getting lower abdomen discomfort from the spasms, you can take the bladder calming medication such as solifenacin or mirabegron. Occasionally bleeding can occur around the catheter and this is also normal.
When you attend for catheter removal, please ensure you have emptied your bowels. If you are constipated then the success after catheter removal reduces because the bowel puts pressure on the water passage and it can be difficult to pass urine.
Try to arrive with a comfortably full bladder (have the flip-flow valve closed for a couple of hours) so that your stay will be as short as possible. The catheter tube will be removed and then when you are ready you will be asked to void urine and the bladder scanner will detect any remaining volume of urine. If the nurse is happy with the results, you will be discharged.
Your bladder emptying will be assessed once the catheter has been removed in clinic (trial without catheter clinic). For this appointment expect to be in the hospital for around 3-5 hours. This will allow time for the catheter to be removed and for an assessment to be made that you are able to empty the bladder.
Within a few days you will be able to resume normal non-strenuous activities and should notice small improvements within 2 weeks, although it may be 3 months before the full benefit is evident. Blood may be visible in the urine and ejaculation fluid. Sometimes, the urinary symptoms get worse before improving and this is because the prostate initially swells.
We may have to teach you the technique of Clean Intermittent Self Catheterisation (CISC) if we think the catheter should be removed but you may have problems with emptying your bladder properly. Although this may sound difficult to perform, most people learn it very quickly. It involves you passing a small, slippery soft plastic tube (the catheter) into the bladder to empty it and then removing the catheter once the bladder is empty. You would only do this when you needed to; in time your bladder would start to work again and your need for CISC would become less and less.
If you cannot re-establish normal bladder emptying we may decide to carry out a cystoscopy (using a telescope to look into the bladder) at a later stage. Some men, about 1 in 50, may need this to be done. At the time a small procedure may be performed in order to improve normal bladder emptying. This might involve releasing some scar tissue in the prostate (formed as a result of the Nanoknife) or cutting through the tight bladder neck in order to allow more of the bladder to empty. Very occasionally some dead tissue or debris within the prostate would have to be removed. These procedures can be done using a telescope and should require no more than a one night stay in hospital. If you need these procedures, they will be explained to you in detail at the time and your consent will be required.
Which medication should I take after the procedure?
It is normal to have some pain or discomfort after operations, and we advise you to take the paracetamol and ibuprofen (if you can take these) painkillers regularly at the full dose for 28 days to help keep it under control. If you are getting symptoms and urgency, frequency, getting up at night, and poor flow worse than before the procedure, continue with these painkillers.
To prevent infection, you will be given a course of antibiotics for 7 days and sometimes longer. Please take these regularly and finish the course. These reduce the risk of infection but not eliminate the risk.
Continue any prostate medication for 28 days. After this, take tamsulosin or alfuzosin every other day for two weeks, then stop it entirely. If the symptoms get worse after stopping, then restart the medication and continue til 3 months after the procedure.
If you are taking finasteride or dutasteride, then stop these after 28 days.
If you are taking bladder calming tablets such as mirabegron, oxybutynin, solifenacin or tolterodine, then stop these after 3 months from the procedure.
Restart blood thinning tablets on the advice of the surgeon.
When can I resume sexual activity, if relevant?
Once the catheter has been removed and you feel comfortable. Do not be surprised if you see blood afterwards and it is painful during orgasm. You can take painkillers such as paracetamol or ibuprofen an hour beforehand and this will help. In order to help with confidence, you may wish to masturbate first before sexual activity with a partner. Regular activity will help recover function that may not be as good as before the procedure. Some men require medication to give the erectile function a boost. Your surgeon can advise on this – usually this is prescribed if there are still significant issues at the 3 months stage.
When can I go back to work?
It would be best to stay off work for 2 weeks. If your catheter is required to be in for 2 weeks then you will need an additional week to stay off work. This is because any kind of activity, even a desk job, can divert energy from the healing process and will delay your recovery.
After this period of time, you can go back to non-strenuous work (e.g., desk job) and then normal physical work activities, if relevant to you, after 4 weeks. You should ask your employer to make reasonable adjustments such as reducing the amount of physical activity and ensuring a toilet is close by.
What exercise can I do after the procedure?
Avoid any exercise for a month after the procedure. During the first month you can go for daily walks of no more than 20 minutes in duration. This is because the pressure on the abdomen can make the prostate swell and bleed and delay your recovery.
In the first month, return to 50% of whatever exercise you normally do. If you get worsening symptoms or bleeding, then avoid this exercise for another 2 weeks and then back to 50% of normal. After this second month, you can go back to 75% of normal exercise for another month. After this, you can return to normal.
How will I be monitored in the future?
After Nanoknife treatment, it is important that you are monitored for a minimum of 10 years by your GP and hospital. Although most men can expect a cure from this treatment, some cancer cells may remain, or the cancer may re-occur.
You will need regular check-ups and PSA (prostate specific antigen) blood tests after prostate cancer treatment. Usually, the PSA will be first tested 3 months AFTER your Nanoknife procedure, then at 3 monthly intervals for the first year. We will ask your GP to take over the PSA monitoring and to update us with the readings. After this time, if the PSA is stable we will advise the frequency of PSA monitoring be reduced to 6 monthly intervals for a period of 2 years, then at annual intervals. You will need to continue being reviewed in hospital annually.
We would anticipate a reduction in the PSA value after Nanoknife. The amount the PSA value may fall by varies from man to man, and depends on how much of the prostate is left behind (we do not yet know the optimal level it may fall by). An MRI scan is done after one year and may sometimes be repeated.
You will also be monitored for any urine or erection problems and offered support or treatment, as necessary. If you experience any difficulties with your erections or urine symptoms please speak to your doctor or contact your nurse specialist.
What are the chances of the cancer recurring?
If your PSA level shows a persistent rise you might be offered an MRI followed by prostate biopsies by your surgeon. If these biopsies show prostate cancer cells the Nanoknife may be repeated. We expect 1 in 5 men to need a second Nanoknife or a different type of focal therapy within 5-10 years. Your suitability for further treatment will be assessed by your surgeon. If further focal treatment is not possible, other treatments that might be considered include surgery, radiotherapy and hormone treatment. Each of these will have different side-effects and cancer control rates which your doctor will discuss.
Comments, concerns, compliments and complaints
Your feedback is important to us. If you have any comments, concerns, compliments or complaints about your care, please let us know as soon as possible. Please speak to one of the ward staff, so that we can help to resolve your concerns quickly. You can also contact your consultant directly by writing to him or her or if you wish, you can contact the complaints team or write to the Chief Executive. Full details of correspondence addresses can be given to you on request.
Any other questions?
We hope this information is helpful. If you have any questions, please ask your doctor or nurse. Further information is also available via the following organisations:
Prostate Cancer UKTel: 0800 074 8383prostatecanceruk.org
Macmillian Cancer SupportTel: 0808 808 00 00macmillan.org.uk
Out of hours, please contact your GP or nearest Accident & Emergency Department
References:
- Hashim Ahmed, Manit Arya, Peter Scardino and Mark Emberton. 2011. Interventional Techniques in Uro-oncology. Chichester, UK: Wiley Blackwell
- Hashim U. Ahmed, Manit Arya, Peter Carroll and Mark Emberton. 2011. Focal Therapy in Prostate Cancer. Chichester, UK: Wiley-Blackwell
Further information
Private referrals
For private referrals, Professor Ahmed works at Cromwell Hospital and Imperial Private Healthcare. Self-pay patients do not need a referral to consult Professor Ahmed and there are competitive self-pay packages offered. Insured patients should check with their insurer. Please use the online booking portal or email the team on london.prostate@gmail.com.
Related
-
Laser for prostate enlargement
Laser treatment for enlarged prostate is an operation that uses a laser to remove excess tissue in the central part of your prostate gland.
-
Steam therapy for prostate enlargement
Steam treatment involves injecting steam into the prostate to destroy enlarged tissue which is causing blockage to urine flow and bothersome symptoms.